Guide to the Light and Shadow of Photon Counting CT
Welcome, fellow creatures of the radiology darkness. I am Count Photon, emerging from my lead-lined reading room to illuminate the mysteries of Photon Counting CT (PCCT)—a technology that, like myself, counts individual particles of light in the darkness. But fear not, dear reader, for the remainder of this educational journey shall be free of supernatural metaphors, focusing instead on the very real science and clinical implications of this emerging technology.
Given the significant influence that photon counting CT currently exerts on clinical decision-making and its anticipated role as the technology driver for the next five to ten years in CT, this serves merely as an introductory overview. Consider this as the first installment of a series that will be further explored on countphoton.com.
Content
- Fundamental Principles of Photon Counting Detection
- Spectral Imaging Capabilities and Clinical Applications
- Virtual Mono-energetic Imaging
- Material Decomposition
- K-edge Imaging
- Spatial Resolution Advances
- Technical Limitations and Implementation Challenges
- Pulse Pileup Effects
- Charge Sharing
- Data Processing Demands
- Critical Analysis: Why Isn’t Everyone Using PCCT yet?
- Economic and Practical Barriers to Adoption
- The Count’s Conclusion
1. Fundamental Principles of Photon Counting Detection
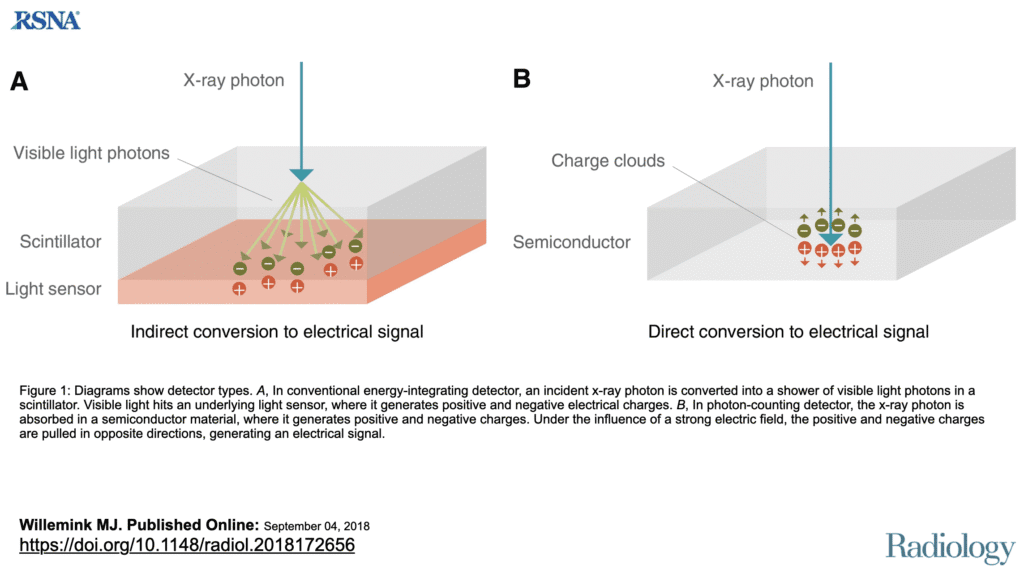
Traditional CT scanners use energy-integrating detectors that convert X-rays to visible light through a scintillator layer, then to electrical signals—a two-step process that inherently loses spectral information. In contrast, PCCT technology employs direct-conversion semiconductor detectors that can detect and count individual X-ray photons1.
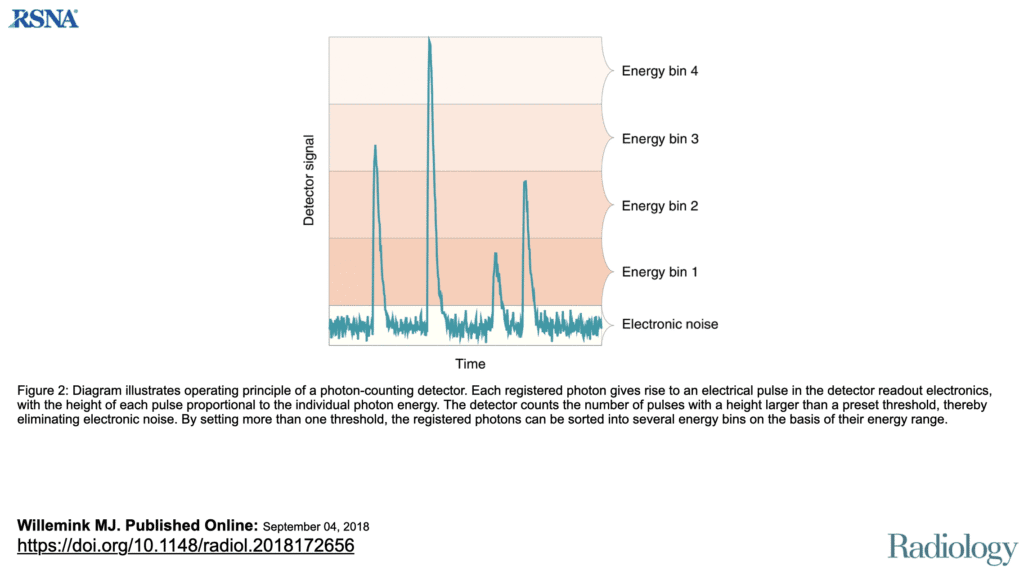
The core components include semiconductor materials such as cadmium telluride (CdTe) or silicon. When an X-ray photon interacts with these detectors, it generates electron-hole pairs that produce electrical pulses. The pulse amplitude directly correlates with the photon’s energy, enabling the system to categorize photons into distinct energy bins—typically ranging from two to seven bins in current clinical systems2.
Photon-counting CT: Technical Principles and Clinical Prospects Martin J. Willemink, Mats Persson, Amir Pourmorteza, Norbert J. Pelc, and Dominik Fleischmann Radiology 2018 289:2, 293-312
This direct conversion architecture eliminates the intermediate scintillator layer, providing several fundamental advantages:
- Complete electronic noise elimination: Energy discrimination circuits ignore signals below predetermined thresholds
- Inherent spectral information: Every acquisition provides multi-energy data without special protocols
- Improved spatial resolution: Smaller detector elements without light spread from scintillators
- Enhanced temporal resolution: Direct conversion enables faster photon processing
Current clinical implementations demonstrate 22-36% noise reduction3,4 and 19-59% dose reduction compared to conventional CT systems5,6,7 though these improvements vary significantly based on specific imaging protocols and clinical applications.
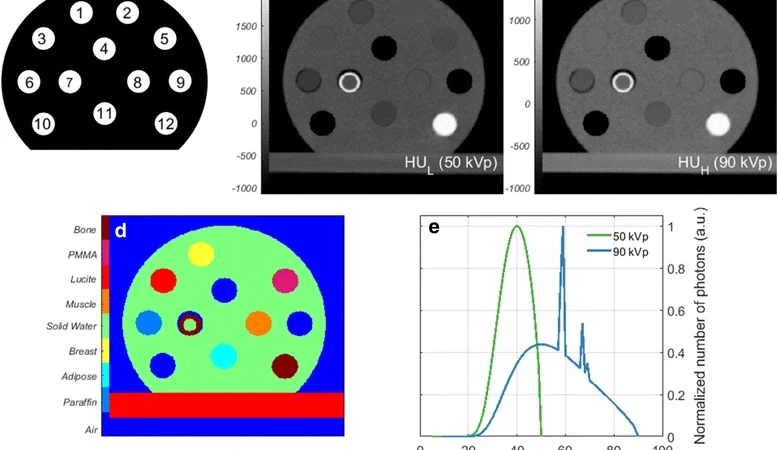
2. Spectral Imaging Capabilities and Clinical Applications
Photon counting computed tomography (CT) inherently captures the energy level of individual photons, enabling it to discriminate between distinct energy “layers” within the detector. This process is known as binning.
Manufacturers of this new CT technology can subsequently determine the number of energy bins they wish to program into their detector. Theoretically, this implies that since the raw data captured by the detector contains the energy-discriminating information, spectral data would be available for every patient.
Photon-counting CT: Technical Principles and Clinical Prospects Martin J. Willemink, Mats Persson, Amir Pourmorteza, Norbert J. Pelc, and Dominik Fleischmann Radiology 2018 289:2, 293-312
PCCT’s inherent spectral capabilities enable multiple advanced imaging techniques from a single acquisition:
Virtual Mono-energetic Imaging
Reconstructions can be generated at any energy level between 40 and 190 keV, optimizing contrast for specific diagnostic tasks. Low-energy reconstructions enhance iodine contrast, while high-energy reconstructions reduce metal artifacts1.
Material Decomposition
Advanced algorithms separate materials based on their energy-dependent attenuation characteristics. Current systems can differentiate:
- Water and calcium for bone density assessment
- Iodine quantification for perfusion evaluation
- Uric acid crystal detection in gout diagnosis
- Fat fraction analysis in liver disease
K-edge Imaging
The technology enables detection of contrast agents based on their characteristic K-edge absorption. While iodine remains the primary agent, research explores gadolinium, bismuth, and gold nanoparticles for targeted molecular imaging applications14.
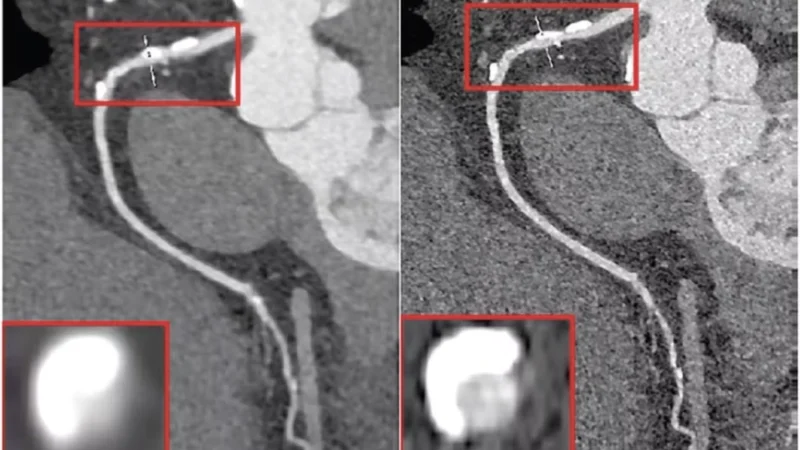
3. Spatial Resolution Advances
This improvement particularly benefits:
- Coronary stent evaluation
- Temporal bone imaging
- Musculoskeletal micro-architecture assessment
- Lung nodule characterization
Clinical PCCT systems achieve pixel sizes of 250 micrometers in standard mode10 and 150 micrometers in ultra-high-resolution mode8,9 compared to conventional CT’s typical 240-500 micrometer resolution.
4. Technical Limitations and Implementation Challenges
Despite compelling theoretical advantages, several technical limitations constrain current PCCT implementations:
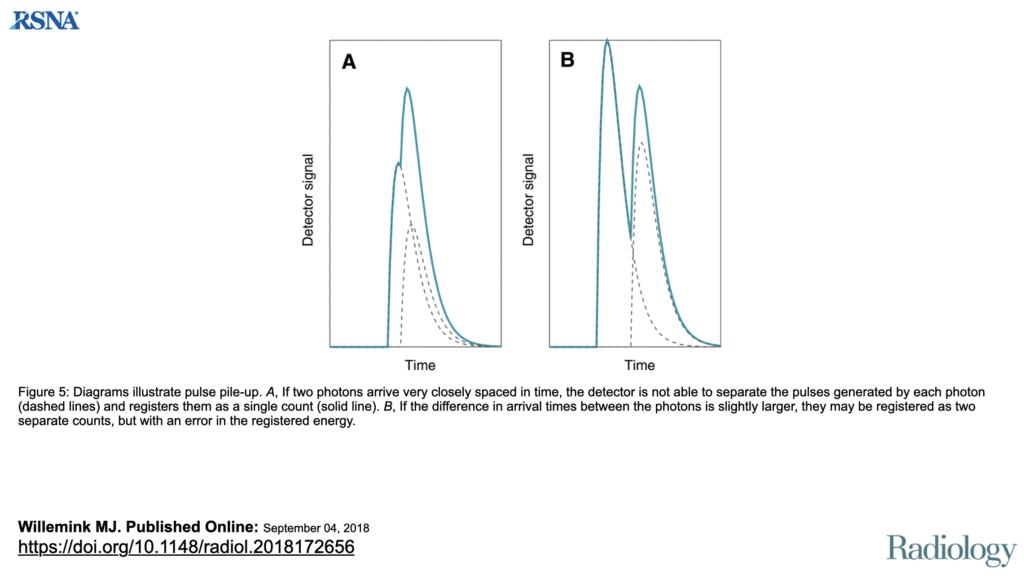
Pulse Pileup Effects
At high photon flux rates (several hundred million photon interactions per mm2 and second)11, multiple photons may arrive nearly simultaneously, registering as single events.
This causes:
- Count loss leading to CT number inaccuracies
- Spectral distortion compromising material decomposition
- Image artifacts in low-attenuation regions
Photon-counting CT: Technical Principles and Clinical Prospects Martin J. Willemink, Mats Persson, Amir Pourmorteza, Norbert J. Pelc, and Dominik Fleischmann Radiology 2018 289:2, 293-312
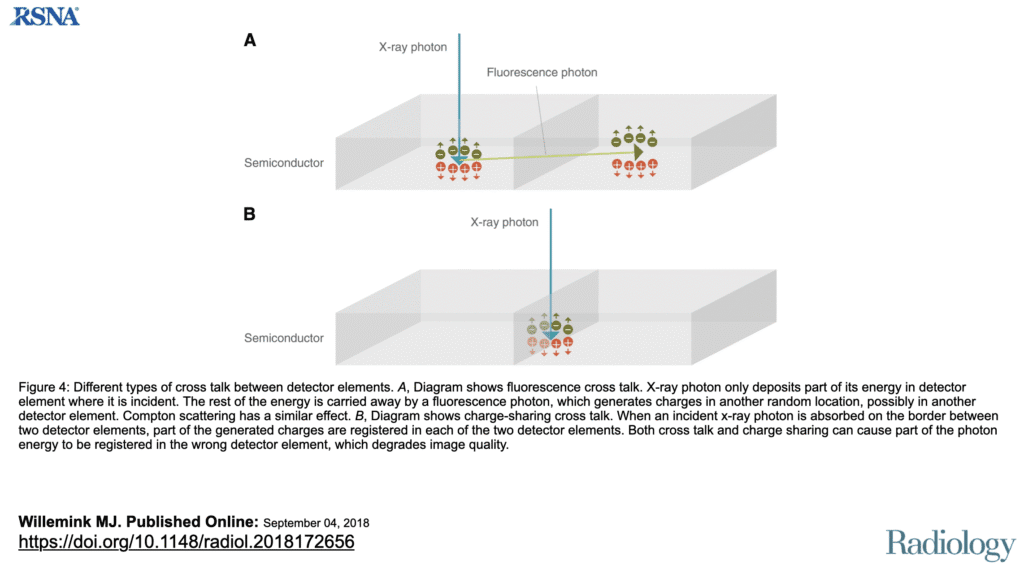
Charge Sharing
When photons interact near pixel boundaries, the generated charge splits between adjacent pixels. This phenomenon:
- Degrades spatial resolution
- Reduces spectral accuracy
- Complicates quantitative imaging applications
Photon-counting CT: Technical Principles and Clinical Prospects Martin J. Willemink, Mats Persson, Amir Pourmorteza, Norbert J. Pelc, and Dominik Fleischmann Radiology 2018 289:2, 293-312
Data Processing Demands
PCCT generates substantially more data than conventional CT:
- Multiple energy reconstructions per acquisition
- Material decomposition maps
- Virtual non-contrast images
- Quantitative spectral parameters
This data volume requires upgraded infrastructure including enhanced PACS capabilities, increased storage capacity, and specialized viewing workstations18.

5. Critical Analysis: Why Isn’t Everyone Using PCCT yet?
Despite theoretical advantages, widespread adoption faces significant obstacles:
- Economic Reality: The 3-5x cost premium cannot be justified without demonstrated outcome improvements and appropriate reimbursement15
- Technical Maturity: Current limitations in count rate capability and charge sharing affect image quality in challenging scenarios11
- Clinical Evidence: Large-scale studies demonstrating improved patient outcomes remain limited
- Workflow Disruption: Integration challenges and training requirements deter many departments18
6. Economic and Practical Barriers to Adoption
Financial Considerations
PCCT systems cost 3-4 times more than conventional CT scanners15:
- Conventional CT: $1-1.5 million15
- PCCT systems: $3-5 million (e.g., NAEOTOM Alpha approximately US$5 million)15
- No specific reimbursement codes exist for PCCT procedures
- Return on investment remains uncertain without premium reimbursement
Infrastructure Requirements
- Upgraded PACS with spectral imaging capabilities
- Increased data storage (estimated 3-5x conventional CT based on multiple energy reconstructions)
- Enhanced reconstruction computing power
- Specialized viewing workstations
- Extended room time for complex reconstructions
Training and Integration
- Radiologists require extensive training in spectral image interpretation
- Technologists need protocol optimization expertise
- Learning curve for clinical proficiency
- Workflow redesign to accommodate longer reconstruction times
Scheduling Considerations
- Longer room time initially (estimated 15-20% increase based on early adopter experience)
- Complex examinations require additional reconstruction time
- Maintenance windows for calibration procedures
Image Interpretation Changes
- Multiple image sets per examination
- Need for specialized viewing protocols
- Learning curve for optimal energy selection
- Integration of quantitative spectral data
Reporting Modifications
- Incorporation of spectral findings
- Quantitative measurements (iodine concentration, Z-effective)
- Comparison with conventional CT appearance
- Education of referring physicians on new metrics
7. The Count’s Conclusion
Dear reader, if you have journeyed this far through the technical forests and clinical castles of Photon Counting CT, Count Photon salutes your dedication to understanding this evolving technology. Like a vampire who has witnessed centuries pass, I encourage you to view PCCT with both ancient wisdom and modern skepticism. The technology offers genuine advances—direct photon detection, spectral information, and dose reduction—but requires careful consideration of costs, limitations, and implementation challenges.
Continue your education, question bold claims, and remember that even technologies counting individual photons must prove their worth in the unforgiving daylight of clinical practice.
Thank you for allowing this old Count to share these insights, and may your future imaging endeavors be filled with clarity, whether achieved through conventional or photon-counting means.
Stay curious, stay critical, and keep learning.
—Count Photon
References
- Willemink MJ, Persson M, Pourmorteza A, Pelc NJ, Fleischmann D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology. 2018;289(2):293-312. DOI: 10.1148/radiol.2018172656
- Flohr T, Schmidt B. Technical basics and clinical benefits of photon-counting CT. Investigative Radiology. 2023;58(7):441-450. DOI: 10.1097/RLI.0000000000000980
- Rajagopal JR, Farhadi F, Richards T, et al. Comparison of Low Dose Performance of Photon-Counting and Energy Integrating CT. Academic Radiology. 2021;28(11):1754-1760. DOI: 10.1016/j.acra.2020.09.006
- Masturzo L, Brunner S, Van de Steene V, et al. Voxelwise characterization of noise for a clinical photon-counting CT scanner with a model-based iterative reconstruction algorithm. European Radiology Experimental. 2025;9:2. DOI: 10.1186/s41747-024-00541-2
- Greffier J, Si-Mohamed S, Guiu B, et al. Potential dose reduction and image quality improvement in chest CT with a photon-counting CT compared to a new dual-source CT. Physica Medica. 2025;120:103334. DOI: 10.1016/j.ejmp.2024.103334
- Mergen V, Sartoretti T, Baer-Beck M, et al. Cardiac imaging with photon counting CT. British Journal of Radiology. 2023;96(1149):20230407. PMID: 37335192
- van der Werf NR, Rodesch PA, Si-Mohamed S, et al. Dose Reduction in Coronary Artery Calcium Scoring Using Mono-Energetic Images from a Novel Dual-Source Photon-Counting Detector CT. Diagnostics. 2021;12(1):8. DOI: 10.3390/diagnostics12010008
- Leng S, Bruesewitz M, Tao S, et al. 150-μm spatial resolution using photon-counting detector computed tomography technology: technical performance and first patient images. Investigative Radiology. 2018;53(11):655-662. DOI: 10.1097/RLI.0000000000000488
- Rajendran K, Petersilka M, Henning A, et al. First clinical photon-counting detector CT system: technical evaluation. Radiology. 2022;303(1):130-138. DOI: 10.1148/radiol.212579
- Sartoretti T, Landsmann A, Nakhostin D, et al. Photon-counting detector CT: early clinical experience review. British Journal of Radiology. 2023;96(1147):20220544. DOI: 10.1259/bjr.20220544
- Danielsson M, Persson M, Sjölin M. Photon-counting x-ray detectors for CT. Physics in Medicine & Biology. 2021;66(3):03TR01. DOI: 10.1088/1361-6560/abc5a5
- Emrich T, Peeler C, Siddiqui AI, et al. Ultrahigh-Spatial-Resolution Photon-counting Detector CT Angiography of Coronary Artery Disease for Stenosis Assessment. Radiology. 2025;310(1):e231956. DOI: 10.1148/radiol.231956
- Graafen D, Emrich T, Halfmann MC, et al. Photon-counting detector CT versus energy-integrating detector CT of the lumbar spine at different tube voltages. European Radiology. 2024;34(1):158-169. DOI: 10.1007/s00330-023-09992-4
- McCollough CH, Boedeker K, Cody D, et al. The technical development of photon-counting detector CT. European Radiology. 2023;33(8):5321-5330. DOI: 10.1007/s00330-023-09545-9
- Canadian Agency for Drugs and Technologies in Health (CADTH). Photon-Counting CT: High Resolution, Less Radiation: Emerging Health Technologies. Ottawa (ON): CADTH; 2024 Feb. PMID: 38546658. Available at: https://www.cadth.ca/photon-counting-ct-high-resolution-less-radiation
- Vecsey-Nagy M, Schoepf UJ, Tremamunno G, et al. Cost-effectiveness of ultrahigh-resolution photon-counting detector coronary CT angiography for the evaluation of stable chest pain. European Journal of Radiology. 2025;182:111807. DOI: 10.1016/j.ejrad.2024.111807
- Hsieh SS, Leng S, Rajendran K, et al. Photon Counting CT: Clinical Applications and Future Developments. IEEE Transactions on Radiation and Plasma Medical Sciences. 2021;5(4):441-452. DOI: 10.1109/trpms.2020.3020212
- Dane B, Bhattacharya I, Ginocchio LA, et al. Photon counting CT clinical adoption, integration, and workflow. Abdominal Radiology. 2024;49(12):4600-4609. DOI: 10.1007/s00261-024-04503-5
Additional Resources
- FDA. FDA Clears First Major Imaging Device Advancement for Computed Tomography in Nearly a Decade. September 30, 2021. Available at: https://www.fda.gov/news-events/press-announcements/fda-clears-first-major-imaging-device-advancement-computed-tomography-nearly-decade
- Siemens Healthineers. NAEOTOM Alpha Technical Specifications. Available at: https://www.siemens-healthineers.com/computed-tomography/photon-counting-ct-scanner/naeotom-alpha